The typical patient with an amebic liver abscess in the United States is an immigrant, usually a Hispanic male, 20–40 years old, who presents with fever, right upper quadrant pain, leukocytosis, abnormal serum transaminases and alkaline phosphatase, and a defect on hepatic imaging study. Roughly 90% of patients with liver abscess are males. The abscess is usually single and is in the right lobe of the liver 80% of the time (Figure 4(d)) (Katzenstein et al., 1982).
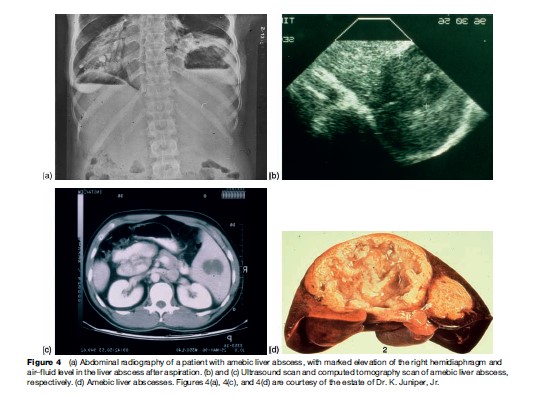
Most frequently, patients will present with liver abscess without concurrent colitis, although a history of dysentery within the last year can often be obtained. Ameba are infrequently seen in the stool at the time of diagnosis of liver abscess (Adams and MacLeod, 1977). Liver abscess can present acutely with fever, right upper abdominal tenderness, and pain, or subacutely with prominent weight loss and, less frequent, fever and abdominal pain. The peripheral white blood cell count is elevated, as is the alkaline phosphatase level in many patients. Early evaluation of the hepatobiliary system with ultrasound or CT is essential to demonstrate the abscess in the liver (Figure 4). The differential diagnosis of the lesion in the liver would include pyogenic abscess (less likely if the gallbladder and ducts appear normal), hepatoma, and echinococcal cyst. Aspiration of the abscess is occasionally required to diagnose amebiasis. (Although ameba are visualized in the pus in only the minority of cases, if the abscess is pyogenic the responsible bacteria will be seen and/or cultured.) Antibodies to E. histolytica are present in the serum of 92–97% of patients upon acute presentation with amebic liver abscess, and therefore are very useful diagnostically. Unusual extraintestinal manifestations of amebiasis include direct extension of the liver abscess to pleura or pericardium, and brain abscess.
In a patient who presents with right upper quadrant pain, an ultrasound, CT, or MRI should be performed to examine the liver and gallbladder. If a space-filling defect in the liver is observed, the differential diagnosis includes: (1) amebiasis (most common in adult males with a history of travel or residence in a developing country), (2) pyogenic or bacterial abscess (suspect in women, patients with cholecystitis, the elderly, individuals with diabetes, and in patients presenting with jaundice), (3) echinococcal cysts (this would be an incidental finding as echinococcal cysts should not cause pain or fever, unless secondarily infected), and (4) cancer. Most patients with amebic liver abscess will have detectable circulating antigen in serum, as well as serum antiamebic antibodies.
How Should Amebiasis Be Treated?
Invasive amebiasis should be treated with metronidazole or tinidazole plus a ‘luminal’ agent such as diloxanide furoate, paromomycin, or diiodohydroxyquin. Metronidazole or tinidazole alone does not eliminate intestinal colonization in up to 50% of patients with invasive amebiasis, leaving patients open to the real possibility of a relapse of invasive infection months later. The majority of patients defervesce after less than 3 days’ treatment with metronidazole. Chloroquine, dehydroemetine, and needle aspiration of the abscess have all been successfully used for the rare patient not responding to metronidazole.
Metronidazole is concentrated in the ameba probably via reduction of its nitro group by ferredoxin or flavodoxinlike electron transport proteins, which maintain a gradient for the entry of the unchanged drug. Metabolic intermediates of metronidazole damage DNA and possibly other macromolecules, and deprive the organism of reducing equivalents by acting as an electron sink.
Future
Providing safe food and water for all children in developing countries would be ideal for prevention of the disease but require massive societal changes and investments. An effective vaccine is less costly and would be a desirable and feasible goal. Continued support of developed countries is essential for the development of effective vaccines and the control of infectious diseases in developing countries.
Bibliography:
- Adams EB and MacLeod IN (1977) Invasive amebiasis. I. Amebic dysentery and its complications. II. Amebic liver abscess and its complications. Medicine 56: 315–334.
- Barwick R, Uzicanin A, Lareau S, et al. (2002) Outbreak of amebiasis in Tbilisi, Republic of Georgia, 1998. American Journal of Tropical Medical and Hygiene 67: 623–631.
- Diamond LS and Clark CG (1993) A redescription of Entamoeba histolytica Schaudinn 1903 (emended Walker 1911) separating it from Entamoeba dispar (Brumpt 1925). Journal of Eukaryotic Microbiology 40: 340–344.
- Duggal P, Haque R, Roy S, et al. (2004) Influence of human leukocyte antigen class II alleles on susceptibility to Entamoeba histolytica infection in Bangladeshi children. Journal of Infectious Diseases 189: 520–526.
- Haque R, Ali IKM, Sack RB, et al. (2001) Amebiasis and mucosal IgA antibody against the Entamoeba histolytica adherence lectin in Bangladeshi children. Journal of Infectious Diseases 183: 1787–1793.
- Haque R, Mondal D, Duggal P, et al. (2006) Entamoeba histolytica infection in children and protection from subsequent amebiasis. Infection and Immunity 74: 904–909.
- Katzenstein D, Rickerson V, and Braude A (1982) New concepts of amebic liver abscess derived from hepatic imaging, serodiagnosis, and hepatic enzymes in 67 consecutive cases in San Diego. Medicine 61: 237–246.
- Haque R, Huston CD, Hughes M, et al. (2003) Current concepts: Amebiasis. New England Journal of Medicine 348: 1565–1573.
- Hughes M and Petri WA Jr (2000) Amebic liver abscess. Infectious Diseases Clinics of North America 14: 565–582.
- Stanley SL Jr (2003) Amoebiasis. Lancet 361: 1025–1034.
- WHO (1997) Amoebiasis. WHO Weekly Epidemiologic Record 72: 97–100.